Am I just being ignored? @lenka-urbandroid
Hello, I think I already mentioned this - I cannot work 24/7. You are not being ignored, we just need to sleep too.
The automatic tracking does not seem to have any data - so probably your wearable did not react to the attempts to connect.
The tracking duration is almost 13 hours. So to get RDI 1, there were probably around 13 SpO2 dips. Is that correct? In the zoomed section, I see 8 of them. 8/13 is approximately 0.6, so rounded to RDI = 1. Does it not match?
Yes sorry first post was almost 2 Days ago
That RDI algorithm confuses the heck out of me. Why not just count all the dips as they go and leave it as such like AHI does. Again RDI confuses me if I have 20bdips in 1 hour then 40 dips 2 hours later then 40 2 hours later and I sleep for 10 hours can’t be that my “RDI” or AHI which is what sleep labs go by be just 10 . It’s not accurate info. ![]()
Yes, from time to time, we need to take a day off. I hope you can understand it.
RDI is an index of distrubances per hour. We decided to go with RDI, some recommend RDI, some AHI - there is no unified guideline, which is better.
According to some sources, using AHI leads to misdiagnoses, so RDI is recommended instead. Why do you think RDI is not accurate?
I don’t know where you got RDI is more accurate than AHI. Federal sleep Lab clinics use AHI, that should give you a hint. RDI throws in rera’s calculation which is dumb pardon my French. A person who can easily have an AHI of 1 can be shown to have an RDI of 15 and freak out thinking he has apnea and what’s causing the little distress ( not the stopping of breathing ) is having asthma or a deviated septum, etc ( nothing really apnea related ). So just imagine someone who actually has apnea and their AHI is 10, RDI can easily show 50 if that said person has a deviated septum, asthma, drank a beer that night, hence for real so ea related stuff OSA, CSA, and Complex, RDI is useless. But if you think differently we’ll you are entitled to that opinion not the fact out there ![]()
I did not say RDI is more accurate than AHI. I said “According to some sources, using AHI leads to misdiagnoses, so RDI is recommended instead.”
So asthma attacks, and trouble breathing leading to a drop in the SpO2 level should not be considered as breath disturbances?
This source says that the AHI misdiagnosis rate is 30%. Sounds like a lot.
“Obstructive sleep apnea (OSA) was initially diagnosed based on the apnea hypopnea index (AHI), but the ICSD-3 has defined the respiratory disturbance index (RDI) as the actual diagnostic criteria.”
The International Classification of Sleep Disorders
And if you have RDI 50 during 8 hours, it means you had approximately 400 dips in the SpO2. Does it not mean your breath disturbance number is high?
No because you couldve easily have had 0 AHI. RERA’s are NOT going to kill you like if you actually stop breathing. No doctor in their right mind would provide you a CPAP machine because of a “sleep disturbance” other than AHI.
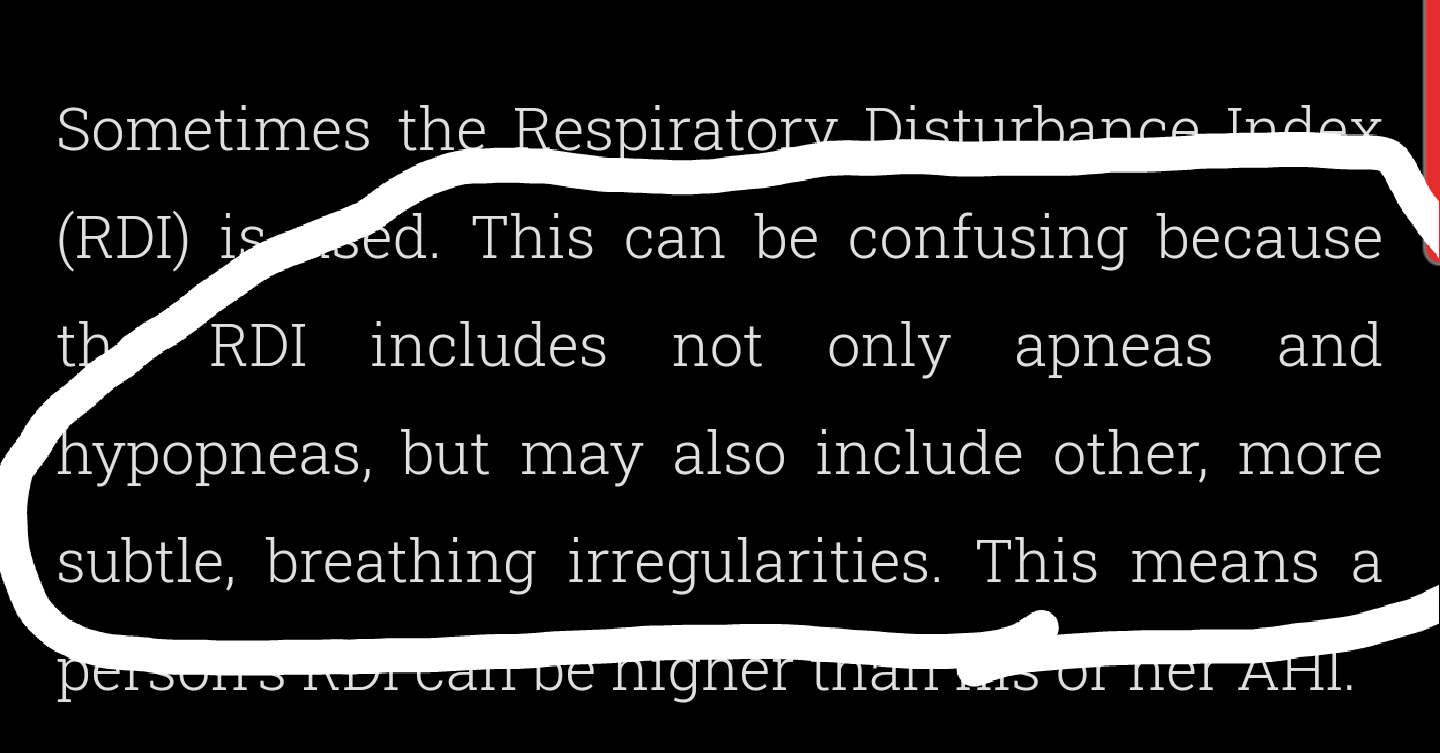
Keyword “confusing” meaning it’s going to throw out a bunch of unimportant stuff that’s going to hinder the actual outcome
RDI is an index of respiratory disturbances. So it does count all breath disturbances. RERA might not kill you but they are respiratory disturbances, hence included in the respiratory disturbances index.
We want to provide our users with information about all respiratory disturbance events. So we use RDI.
So is The International Classification of Sleep Disorders wrong?
The information about switching from AHI to RDI is from 2022.
I give you an answer you ask me another that’s been already answered. You didn’t care to read what I shared and see it’s past 2022. I care about the Harvard study more than the study you posted. Harvard has one of the biggest Sleep disturbances training centers. But like I said before, disturbances are not going to kill you but muddle the actual important information because it’s thrown in the mix. Going to confuse all users who don’t have a bleep what truly RDI is doing.
I’m not here to change your mind, I’m here presenting you facts. It’s your app at the end you put in it what you feel is best. But like I said you are only entitled to your opinion not the facts at hand.
I don’t know if the international classification of sleep disorder is right or not. But they are NOT the who’s who when testing comes. Anyhow that’s all I’m presenting. Use it as you wish ![]()
I mentioned my source is from 2022, because the Harvard source you posted is from 2021. I did not find any newer study recommending going back from RDI to AHI. Do you have anything newer? Could you share it?
If you have 400 episodes per night (even if all are RERAs), you might not qualify for CPAP, but it might be worrisome enough to see a doctor and consult it.
You might consider hypopneas or RERAs as less severe if you already have Apnea. And you are right, Apnea is worse. But that does not mean others are not interested in less severe breath disturbances, or wish to be aware about them.
I posted your suggestion on our suggestion forum to use AHI. We have several thousands of Apnea-diagnosed users we know of, and probably tons of others, who did not tell us. If more users show their wish to switch to AHI, we will definitely consider it.´
Like I stated before even those with apnea, if they are not knowledgeable of what RDI is throwing at them which 99% of the time it will be rubbish Rera’s stuff, they can easily panic and start calling their doctors, get anxious, etc etc. causing more damage than good for something insignificant.
This was supposed to be sent already for some reason it was saved in drafts ![]()
Anyhow last night I crashed without turning sleep tracker on, but it didn’t record anything and ring had charge when I woke up ![]()
If the tracking does not start automatically, either the wearable did not react to the attempts to connect, or there were too prominent awake-like events. I cannot tell without a log (Left ≡ menu → (?) Support → Report a bug).
What is recording volume threshold for? Phone is picking up my wife’s snoring this muddling my stats. She sleeps a good 10ft away from me
The sound recording threshold decides how loud sounds will be recorded.
The program cannot differentiate between the snoring of each individual - which is currently technically impossible. This would require collecting several hundreds of thousands of samples from each user, and then tailoring a special version for each user.
What would be a good number if she’s 10ft away to just “possibly” only catch me if I snore?
This is highly individual and fully depends on the acoustic parameters of the room you sleep in and the level of sound you two produce while sleeping.
There is no way this could be automated.
You will have to try to adjust the levels. If you need fewer recordings, increase the recording threshold in small steps (let’s say in steps of 5%).
How da heck do o know if I’m premium member?
Directly at the top of the Left menu, you see Sleep as Android label.
If it is a BETA release, you have “Sleep as Android β”.
If is is a premium version, you have “Sleep as Android ![]() ”.
”.
BETA premium looks like this: